Darren Berman, MD
Fostering Innovation in Congenital Interventional Cardiology
Since joining Children’s Hospital Los Angeles in August as the Director of Congenital Interventional Catheterization, Darren Berman, MD, has been expanding the scope of the Interventional Catheterization Program to include many of the newest catheter-based treatments for children and young adults with congenital heart disease.
Dr. Berman—who completed his residency and pediatric cardiology fellowship at Children’s Hospital Los Angeles—has participated in national trials of innovative pediatric devices throughout his career. Below, he shares the latest on new devices in development, including the team’s recent first-in-human procedure.
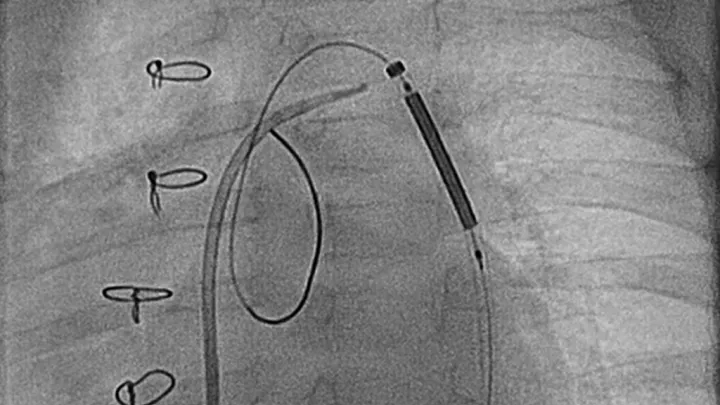
Your team recently performed the world’s first-ever implant of a novel stent for infants. How does it work?
One of the limitations of currently available stents is that they require large-sized delivery systems to implant the stent within a blood vessel. Essentially, this makes it impossible to safely use those stents in small children, infants and neonates.
A company in California has now developed a novel stent and delivery system that is specifically made to fit into a neonate’s small-sized blood vessels. As the baby grows, the stent can be expanded via a repeat catheter procedure. It’s designed to be expanded all the way to adult size and last a lifetime.
This new technology is currently being evaluated as part of a multicenter early feasibility study at four sites around the country. I am honored to represent this study as the national principal investigator. We did the first-in-human implant of this device here at Children’s Hospital Los Angeles on Feb. 1, in a 5-month-old infant with re-coarctation of the aorta.
This is really an unmet need in the pediatric population, so we’re thrilled to be leading this study.
What other new technologies are on the horizon?
One of the clinical trials we’re joining is evaluating a bioabsorbable device that closes an atrial septal defect (ASD)—a hole between the upper chambers of the heart.
We already have devices that close an ASD, and they work very well. But they’re made of soft metal meshwork and non-resorbable materials. When placed across the hole, that metal mesh remains in the heart for the rest of the child’s life, which can be a potential issue down the road.
An important question that many of us have asked is: Can we use a device made of bioabsorbable materials instead? The idea is to put in the device, close the hole and allow the patient’s own tissue to grow over that device. Over time, the device would simply be resorbed by the body. The goal is to leave less of a footprint inside the heart, and that’s what this trial is evaluating.
Another new device we now have available is the Harmony valve. This was recently approved by the Food and Drug Administration and will allow us to replace a child’s pulmonary valve via a catheter procedure instead of surgery.
Talk about the team’s work with transcatheter closure of patent ductus arteriosus (PDA) in premature babies.
We now have the first FDA-approved transcatheter device, the Amplatzer Piccolo Occluder, that can close a PDA in premature infants without surgery. It’s a pea-sized device approved for babies weighing as little as 1 ½ pounds.
Before coming to Children’s Hospital Los Angeles, I was honored to be involved in the clinical device trial that led to the Piccolo Occluder’s FDA approval in 2019. When I arrived here, the interventional cardiology team had already been using this relatively new device in premature infants who were slightly larger. We’re now working with our colleagues in Neonatology to begin safely offering this procedure to the smallest, most fragile low-birthweight babies.
There’s been a trend toward conservatively managing PDAs in preemies. Is it better to close them?
This is a great question, and it’s an ongoing debate in neonatology. For a while, many of these babies had their PDAs surgically repaired, and then the management paradigm swung to favoring more conservative management.
Now that we can close the PDA without surgery, we’re motivated to start a prospective, randomized clinical trial to answer this important question. In conjunction with our Neonatology colleagues, it’s going to include 18 to 20 centers across the country, including Children’s Hospital Los Angeles.
We want to see if earlier closure with this device improves babies’ respiratory status and helps them come off mechanical ventilation faster. I am hopeful that it does, and there are several retrospective studies that support that, but we need to prove it.
What is the biggest challenge now for congenital interventional cardiology?
For decades, we were focused on refining techniques to help keep our patients alive. But as we’ve gotten better at that, there’s a bigger focus now on quality of life. The challenge now is: How well can we fix our patients’ congenital heart disease so they can live as close to a normal life as possible?
Technological advancements will help, but collaboration is critical. We need to bring all of our minds together, across subspecialties, to maximize the long-term quality of life for the children we care for.
Why did you want to return to Children’s Hospital Los Angeles?
I grew up in Southern California, and both my wife and I consider this area home. This is one of the top-ranked children’s hospitals in the country, and the Heart Institute has been an absolute leader, both in the U.S. and in the world. I trained here for six years, so I was very familiar with the exceptional level of care and dedication here.
We have an incredible team in the Cath Lab that includes four interventional cardiologists—myself; Cheryl Takao, MD; Patrick Sullivan, MD; and Neil Patel, MD—and cardiovascular technicians, cardiac nurses and dedicated cardiac anesthesiologists. In addition, we have an excellent and supportive cardiothoracic surgical team. This partnership between the Cath Lab and surgical team is essential when performing these highly complex and sometimes high-risk procedures. It’s a collaborative culture, and I’m excited to be part of it.