New Guidelines for Hamstring Lengthening and Guided Growth Surgery
For the past several years, Robert Kay, MD, has been part of an international group of experts with an ambitious goal: shaping the future of orthopedic care for ambulatory children with cerebral palsy.

“There’s so much variation in how surgeons approach these complex patients,” says Dr. Kay, Chief of Orthopedic Surgery and Director of the Jackie and Gene Autry Orthopedic Center at Children’s Hospital Los Angeles. “Our goal is to provide consensus guidelines—not one person’s opinion—to aid surgeons in their clinical decision-making and help ensure the best care for each child.”
The group, which includes 16 surgeons from 15 leading centers in North America, Europe and Australia, recently published guidelines for two types of surgeries designed to address knee problems in children with cerebral palsy: hamstring surgery and anterior distal femoral hemiepiphysiodesis (also called “guided growth”). Both papers were published in the Journal of Children’s Orthopaedics.
Dr. Kay — who served as lead author on the hamstring surgery paper and a senior author on the guided growth publication — shares some of the group’s key recommendations.
Hamstring surgery
Hamstring lengthening is one of the most common surgeries to address crouch gait, but indications for this procedure have changed in recent years, Dr. Kay says. The panel agreed that:
- A thorough gait evaluation is key. “You can be fooled just on physical exam in thinking a patient’s hamstrings are tight,” Dr. Kay says. “Computerized hamstring modeling data from a gait lab are really helpful in determining whether a child is a good candidate for this surgery.”
- Repeat hamstring lengthening has inferior results. A child’s crouch gait can sometimes recur after an initial hamstring lengthening. But the panel agreed that a repeat lengthening is often not successful. For example, Dr. Kay’s team published a paper several years ago showing that while a first hamstring lengthening had a 71% success rate in straightening a child’s knees, that success fell to just 28% with a second procedure.
- Hamstring lengthening isn’t enough to correct knee flexion contractures. “When contractures are greater than 10 degrees, an isolated hamstring lengthening doesn’t sufficiently address the problem,” Dr. Kay says. “You need to think about doing an osseous procedure around the knee as well.”
Hamstring transfer remains controversial. Although hamstring transfer surgery offers some theoretical advantages over hamstring lengthening—with the idea that it would lessen post-operative anterior pelvic tilt—the panel concluded that data do not yet show that it has better outcomes than hamstring lengthening.
“Hamstring transfer is a much bigger, more complicated and painful surgery,” Dr. Kay says. “There may be a role for it down the road, but right now the data don’t support it.”
- Surgeons should not lengthen lateral hamstrings. The group was unanimous in reporting that they “rarely, if ever” perform isolated lateral hamstring lengthening. There was also consensus that indications for combined medial and lateral hamstring lengthening are very limited in children who walk—those functioning at Gross Motor Function Classification System (GMFCS) levels I-III.
- It’s important to minimize the number of surgical sessions for a child. Hamstring surgery is rarely performed in isolation. The group recommended simultaneously addressing contractures and bony deformities at other levels, as well as lever-arm dysfunction, in a single-event multilevel surgery.
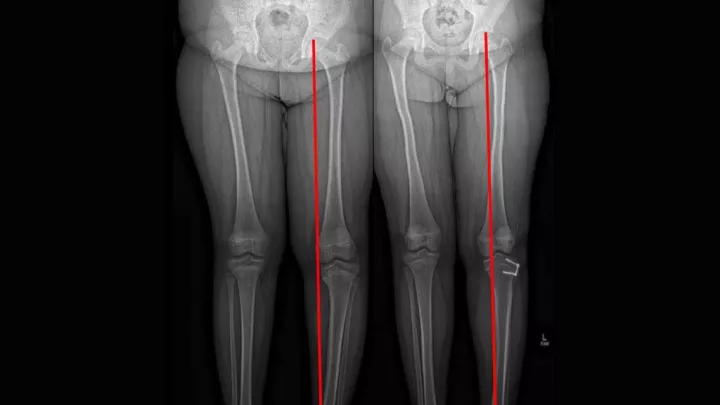
Guided growth surgery
Anterior distal femoral hemiepiphysiodesis was first reported as a method to straighten out knee flexion contractures without cutting into the bone nearly 15 years ago, but it has become much more common in recent years as surgical techniques have evolved. The group agreed that:
The surgery is effective in children with a wide range of walking abilities. Guided growth can be indicated in children at GMFCS levels I-IV—from those who walk in all settings without help to those who only walk short distances at home with assistance.
One advantage is that it’s a low-risk procedure, with small incisions, Dr. Kay adds. Patients are able to start walking the same day as surgery.
- It’s best for contractures between 10 and 20 degrees. The panel could not reach consensus on whether the procedure should be done for knee flexion contractures outside that range, but members agreed that it is not indicated for those larger than 30 degrees.
- Percutaneous screws are preferred over anterior plates. This newer technique—which Dr. Kay helped to popularize in recent years—results in far less postoperative pain than the older screw-and-plate constructs.
- Children should have two years of remaining growth. “The surgery can be a very good option for adolescents who are still growing,” Dr. Kay says. He adds that guided growth is rarely done in children under 10.
What’s next?
The panel is now working on a consensus paper for foot and ankle surgeries in ambulatory children with cerebral palsy. Long term, the group hopes to do more prospective data collection and potentially create a registry to better track and study outcomes data from these procedures.
“It’s really important for surgeons to work together to continually optimize care for these patients,” Dr. Kay says. “Improving a child’s ability to walk has a major impact on the quality of life for that child and family. This is something that will affect them for the rest of their lives.”