
Flat Heads in Babies
Positional Plagiocephaly vs. Lambdoidal Synostosis
In 1992, the American Academy of Pediatrics recommended that infants should sleep on their backs to reduce the risk of SIDS (sudden infant death syndrome). This launched the "Back to Sleep Campaign" and a dramatic increase in the number of children presenting with positional plagiocephaly. Positional plagiocephaly can be confused with lambdoidal synostosis, which also causes flattening of the back of the head. Referrals for positional plagiocephaly and “rule-out craniosynostosis” are one of the most common referrals to a pediatric neurosurgeon or craniofacial plastic surgeon.
Clinical Presentation of Positional Plagiocephaly vs. Lambdoidal Synostosis
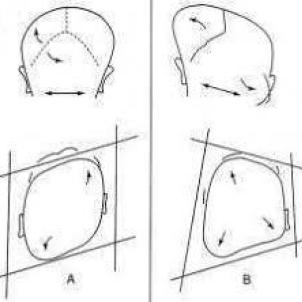
Positional plagiocephaly can typically be diagnosed by an experienced practitioner with a thorough history and clinical exam without the need for X-rays or other imaging, such as CT1, 3. Infants with positional plagiocephaly typically have a normal head shape at birth. A small number of infants may have positional plagiocephaly at birth, typically caused by position in the womb, and it usually resolves itself by 6 weeks of age. In most cases of positional plagiocephaly, the flattening is a result of some infants’ preference for sleeping on their backs with their heads turned consistently in the same position. Positional plagiocephaly is frequently found in infants with torticollis as they have difficulty turning their heads. The flat area may develop very quickly over several months, typically between 2 and 6 months of age, and typically is the most severe at about 4-5 months of age, before the child has started rolling consistently and is no longer sleeping on his or her back. The characteristic parallelogram head shape of positional plagiocephaly is easily identified. There is anterior displacement of the ipsilateral ear and ipsilateral frontal bossing. When looking at the infant’s head from behind, the ears will appear level3 (Figure 1A).
Lambdoidal synostosis results from premature closure of the lambdoidal suture, in contrast to positional plagiocephaly, where all the cranial sutures are open4. The lambdoid suture runs bilaterally from the posterior fontanelle to the asterion, which is located just behind the ear. This is the least common type of craniosynostosis, representing less than 5% of all types of single-suture craniosynostoses5. While typically unilateral, bilateral lambdoidal synostosis can occur as well, causing bilateral occipital flattening. In contrast to positional plagiocephaly, the head shape is usually not normal at birth and gets progressively worse over time. In unilateral lambdoidal synostosis, the affected side of the cranium is typically flat posteriorly, with inferior and posterior displacement of the ipsilateral ear and mastoid bone accompanied by bulging of the contralateral parietal region and frontal region resulting in a trapezoidal shape of the head3,5 (Figure 1B).
Treatment of Positional Plagiocephaly vs. Lambdoidal Synostosis

Positional Plagiocephaly: The risk of positional plagiocephaly can be reduced through a few simple measures4:
- Encourage plenty of supervised playtime on the baby’s tummy. This helps build and strengthen neck, shoulder and arm muscles.
- Encourage parents to change the direction in which the baby is lying in the crib on a regular basis to ensure the baby is not always resting on the same part of the head.
- Encourage parents to change the location of the baby’s crib in the room so that the baby must look in different directions to see the door or the window.
- Encourage parents to avoid having the baby spend too much time in car seats, carriers and bouncers while the baby is awake.
Once a child is able to roll and sit independently, the deformity typically begins to improve. Although it may not resolve completely, the remaining flattening is usually minor and covered with hair as the child grows. The frontal differences are often minimal and tend to resolve completely over time.
If the problem fails to resolve as the child develops, the parents or guardians will be given a referral to see a specialist, such as a pediatric neurosurgeon or craniofacial plastic surgeon. The specialist will review the infant’s history, perform a thorough evaluation and discuss a treatment program, which may involve a positional molding helmet or band therapy2,6. Helmet therapy is typically most effective when done before 6-9 months of age because the bone of the skull is thin and responsive to external forces. Rapid head growth at this age also enhances the effectiveness of the helmet. After 1 year of age, helmet therapy is much less effective due to the thickness of the skull and the slowing of head growth6.
Lambdoidal synostosis is treated surgically by a specialized team of craniofacial plastic surgeons and pediatric neurosurgeons. Both open and minimally invasive or endoscopic techniques have been described5. Endoscopic surgery is typically done prior to 3 months of age and is followed by a course of helmet therapy. Many open surgical techniques have been described for correction of lambdoidal synostosis depending on the severity of the deformity. Open surgery is typically done around 6-9 months of age.
About the Authors
Susan Durham, MD, MS
Chief, Division of Neurosurgery; Attending Surgeon, Children’s Hospital Los Angeles
Professor of Clinical Neurological Surgery, Keck School of Medicine of USC

Mark Urata, MD, DDS
Chief, Division of Plastic and Maxillofacial Surgery; Attending Surgeon, Children’s Hospital Los Angeles
Professor of Clinical Surgery; Audrey Skirball Kenis Endowed Chair and Chief, Division of Plastic and Reconstructive Surgery, Keck School of Medicine of USC


