Does Piccolo PDA Closure Improve Outcomes for Babies?
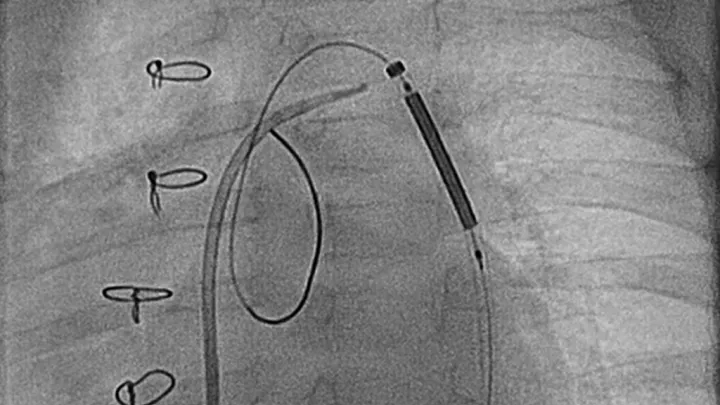
It’s been four years since the Food and Drug Administration approved a tiny, pea-sized device called the Amplatzer Piccolo Occluder—a minimally invasive transcatheter treatment for closing a patent ductus arteriosus (PDA) in premature infants as small as 700 grams.
But while the Piccolo device was shown to be safe and effective at closing these PDAs, an important question remains unanswered: Does this closure lead to better outcomes for babies?
That question is the subject of a new, randomized controlled clinical trial at Children’s Hospital Los Angeles. The multicenter study—funded by the National Institutes of Health and led by Nationwide Children’s Hospital—will directly compare conservative medical management and Piccolo PDA closure.
“In the U.S. and across the world, there’s a major debate over how to best manage the PDA in extremely premature babies, and there’s significant variability across institutions,” says Darren Berman, MD, Director of Congenital Interventional Cardiology at Children’s Hospital Los Angeles and the national lead for interventional cardiology for the trial. “The goal of this study is to provide more clarity on the best approach for these fragile patients.”
A controversial question
An opening between two blood vessels leading from the heart, the ductus arteriosus is critical for fetal circulation and normally closes shortly after birth. The more premature a baby is, though, the more likely it is that the ductus will remain open.
Until about 15 years ago, the accepted treatment for a PDA in premature infants unresponsive to medications was to close it surgically, often as soon as possible. But after studies found that babies who underwent surgical closure did not have better outcomes, the pendulum swung toward conservative medical management.
“Surgery is effective at closing the ductus, but it is invasive and generates a lot of inflammation. It’s a big stress on the baby,” says Shahab Noori, MD, MS, Division of Neonatology Section Head, Clinical Research, in the Fetal and Neonatal Institute, and a site Co-Principal Investigator with Dr. Berman. “And studies have shown that it doesn’t lower the baby’s risk for bronchopulmonary dysplasia, which is the major lung complication of prematurity.”
But as surgery fell out of favor, that created a new challenge: what to do when a baby’s condition continues to worsen despite medical management. An open ductus can result in too much blood flow to lungs, causing difficulty in gas exchange and necessitating increased ventilatory support. That extra blood flow is also “stolen” from the systemic circulation, which can result in additional problems for the babies.
If and when to call the surgeon—or continue medical management—has been the subject of intense debate ever since.

“While many of these premature babies can manage with a PDA and eventually get better, there’s a good proportion who just continue to get worse from a lung standpoint, as well as their other organs,” says Dr. Noori. “Do you wait it out and hope it gets better, or take the risk of surgery? That’s the challenge, and everyone has a different answer.”
The approval of the Piccolo device presented a new alternative: closing the ductus via a catheterization procedure.
“Now we have this option that is less invasive, with less inflammation,” he adds. “If we close the PDA in that way, does that then make a difference for these babies’ outcomes? That’s what we need to learn, and that’s why this is such an important study.”
Comparing two treatment paths
The clinical trial will enroll 240 patients at 20 centers across the U.S., including Children’s Hospital Los Angeles. Enrollment at CHLA is expected to begin in March.
Eligible patients must have been born at less than 28 weeks gestation; have a large, hemodynamically significant PDA at 1 week of age; and be on a ventilator. Participating patients will be randomized into one of two groups:
- A catheterization procedure to close the PDA, using the Piccolo device
- Continued medical management
Investigators will then follow those patients to see which group comes off of the ventilator fastest. The study’s primary endpoint is number of ventilator-free days in the 30-day period after patients are randomized.
The trial will also measure several secondary endpoints, including neurodevelopmental assessments and cardiac outcomes such as pulmonary hypertension.
Dr. Berman notes that extremely premature babies often need a ventilator for multiple reasons, not just a PDA. By focusing only on babies with large PDAs, the team hopes to better pinpoint the impact of closing the ductus.
“We know that a large PDA can place a significant hemodynamic burden on any patient, but it’s been unclear exactly what the implications of that are in this population,” he says. “My hope is that this study will help answer that question, and that this new device can offer a better option for these extremely premature babies.”